Translational Perioperative and Pain Medicine (ISSN: 2330-4871)
ARTICLE DOI: 10.31480/2330-4871/075
CASE REPORTOPEN ACCESS
Retrograde Venous Catheterization Needle Puncture Technique: A Case Report
Tiegang Wei* and Xuefeng Hu
Department of Anethesiology, Haida Hospital, Weihai, China
Tiegang Wei, MD, Department of Anethesiology, Haida Hospital, Weihai, China, E-mail: 13604637421@163.com
Editor: Renyu Liu, MD, PhD, Associate Professor, Department of Anesthesiology and Critical Care, Perelman School of Medicine at the University of Pennsylvania, 336 John Morgan building, 3620 Hamilton Walk, Philadelphia, PA 19104, Phone: 2157461485, E-mail: liur@uphs.upenn.edu
Received: July 15, 2018 | Accepted: October 19, 2018| Published: October 22, 2018
Citation: Wei T, Hu X. Retrograde Venous Catheterization Needle Puncture Technique: A Case Report. Transl Perioper & Pain Med 2018; 5 (4):89-91.
Abstract
Conventionally, the direction of venipuncture that we see is along the vein centripetal direction. Here, we report a retrograde venous puncture (puncture from the proximal end to the distal end) and placement of an intravenous indwelling needle. This case report describes the advantages of retrograde puncture to significantly increase the success rate of puncture.
Keywords
Indwelling needle, Retrograde puncture, Puncture success rate
Introduction
Tumor patients often require a long period and frequent chemotherapy. Due to repeated puncture of peripheral veins and drug effects, the destruction of peripheral blood vessels severely results in a decrease in the success rate of venous puncture. In this article, we discuss a case that demonstrates the feasibility of retrograde venipuncture and the potential importance of increasing the success rate of puncture.
Case Description
Since there is no identifiable or confidential information related to patient care, internal review board exemption is waived. Recently, our hospital received a male patient with lung cancer, lung cancer staging T3N1M1. The patient had left peripheral venous veins open at the dorsal aspect of the left forearm wrist during admission. Unusually, the indwelling catheter was punctured in the opposite direction from the traditional puncture (Figure 1).
Figure 1: The venous indwelling catheter is placed from the proximal end to the distal end in the basilica vein of the patient's left forearm.

Detailed medical history and related medical records: According to standardized treatment of lung cancer, the patient needs to undergo 4 to 6 cycles of chemotherapy (about 1 to 2 years).
It seems that retrograde venous puncture not only improves the success rate of puncture, but also keeps the venous indwelling needle longer, easier to fix and reduce drug seepage.
Discussion
The chemotherapeutic drugs can be very irritable to the vein and often need long term therapy [1], they can induce significant phlebitis, perivenitis, or local tissue necrosis. Repeated intravenous punctures further increase the damage of the vein wall. The well-placed and easily punctured peripheral venous blood vessels are injured one after the other with the increase in the number of chemotherapy, resulting in a gradual decrease in the success rate of veno-puncture and an increase in the risk of chemotherapeutic drug leakage or failure to complete the chemotherapy process.
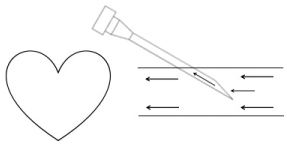
Retrograde venipuncture can increase the success rate of puncture: With forward puncture, the direction of needle travel is the same as the direction of blood flow. The blood will not be traced back to the needle [2], resulting in insufficient blood flow in the thin distal blood vessels. Blood will not flow back to the needle (Figure 2). Puncture when the needle was inserted into the lumen of the blood vessel, there was no apparent fall and it could not be judged whether the needle had entered the blood vessel and whether it continued to enter the needle, causing the needle to fail; at the same time, the patient fisted in the forward puncture, and the dorsal vein was in the metacarpal bone. Hide deeper, not fully exposed, more difficult to puncture. With retrograde puncture, the direction of needle travel is opposite to the direction of blood flow, the needle is more likely to return to the blood (Figure 3), and the dorsal palm vein is exposed more fully [3], the success rate of the puncture is greatly improved. At the same time, the patient is half-fisted in the retrograde puncture and the back of the needle is relatively flat, the skin is tighter, the blood vessels are easier to fix, and the tight parts are easy to grasp. During the puncture and fixation process, the needle handle is in the middle of the back of the hand, avoiding the metacarpophalangeal joint, and the puncture side of the patient is also in a comfortable position, shortening the puncture time and improving puncture success rate [4,5].
Figure 2: The venous indwelling catheter/needle is placed in the same direction as the blood flow, and the blood may not easily enter the intravenous indwelling catheter/needle.
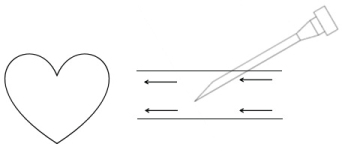
Figure 3: The venous indwelling catheter/needle is placed in the opposite direction to the blood flow, and the blood is more likesly to enter the intravenous indwelling catheter needle.
Retrograde venous puncture can reduce the rate of exudation of drug: When antegrade venipuncture is performed, the exposed part of the scalp needle can easily cause the displacement of the tip of the needle close to the vessel wall or the needle. Therefore, the patient should try to control the position of the metacarpophalangeal joint, otherwise it is easy to mechanical movement, induced drug leakage; and retrograde puncture can increase the length of the needle into the blood vessels, and the needle handle and needle stem are fixed in the back of the hand, not in the knuckle. Due to reduced influence of the activity of the affected joint, but also reduce the possibility of needle slippage, thereby reducing drug exudation rate. In addition, when the retrograde puncture was performed, the patient showed a half-sweeping fist and the palm vein venous network was well exposed. By changing the puncture direction, the same vein was used for those who often required intravenous infusion, but it was equivalent to more intravenous veins, it can effectively avoid the vascular hardening, clogging, and even necrosis caused by repeated punctures, and greatly reduce the phlebitis and drug exudation induced by mechanical reasons [6].
Retrograde venous puncture does not affect the infusion process: The fluid pressure of the infusion system formed by the combination of hydrostatic pressure and atmospheric pressure is higher than the venous pressure of the human body, therefore, the solution can enter the human body directly through the infusion system. It is inferred from the common sense that retrograde puncture will affect the direction of the needle and the direction of blood flow, the number of drops will be affected and the infusion will not proceed smoothly. In fact, because the central venous pressure of the human body is less than the liquid internal pressure of the infusion system, the fluid of the retrograde puncture infusion can completely enter into the blood vessel with the help of the pressure difference. Anatomy principle: Since the venous valve of the human body is open to the heart, blood reflux does not occur after venous return, and accumulation of blood at the drooping position or end of the human body under gravity is also avoided. The venous valve does not allow the fluid to be transported by the retrograde puncture to flow back, ensuring that the fluid flow is consistent with the direction of blood circulation. In addition, a good reticular vein network of hands and feet can easily connect deep veins to the return of the heart. The deep veins and the dorsal veins of the hands are quite anastomosis. The superficial veins of the back of the palm and the back of the fingers are distributed in a reticular pattern,diameter 1.2 ~ 4.0 mm, and the infusion needle diameter is generally 0.6 ~ 0.7 mm. So whether using antegrade or retrograde puncture, can return to the heart through the venous system. Therefore, the use of retrograde puncture does not affect the return of blood and has no effect on the smooth infusion [7].
In our hospitals and many hospitals, the peripheral veins can be used as a route for the administration of small stimulating chemotherapy drugs. In response to the choice of chemotherapy route, we have conducted a multidisciplinary discussion of related issues and consulted the relevant literature: central vein or peripheral vein, depending on the purpose of chemotherapy and the type of chemotherapy drug used; Drugs that require frequent chemotherapy (advanced patients) and chemotherapy drugs with greater peripheral vascular stimuli should be administered via central venous; In the chemotherapy of bowel cancer, continuous infusion of FU must be administered intravenously in the center; Palliative intravenous chemotherapy in patients with advanced disease, subcutaneous implanted infusion port is the best choice. However, if only postoperative adjuvant chemotherapy, such as the XELOX regimen, oxaliplatin is given intravenously every 3 weeks, the peripheral vein is sufficient to complete the postoperative chemotherapy process without causing severe venous injury.
In addition to the medical technology itself, the patient's financial affordability is also an important factor affecting the choice of chemotherapy pathways.
Although the latest guidelines NCCN recommend central vein or PICC as the preferred route of chemotherapy, there are some practical reasons why attending physicians often fails to implement optimal treatment options. Such as the implanted intravenous infusion port that has emerged in recent years, because of its low risk of infection, convenience for patients (does not affect bathing and swimming), protection of blood vessels, simple care, long service life, the technology is subject to clinicians and patients favor. However, due to its high cost, many patients are discouraged.
The special feature of this case is that the economic factor causes the patient to reject the higher-cost central venous catheterization, and the attending physician can only use the peripheral vein for chemotherapy. With the progress of cancer treatment, the contradiction between economic factors and treatment has become more and more prominent. At the end of the tumor, many patients can only supplement glucose for life reasons for economic reasons.
In addition, the medical level of heterogeneity in different regions, the different educational level of patients and the communication effect between doctors and patients will determine the final treatment options.
In conclusion, the retrograde puncture technique provides an alternative option for selecting blood vessels and solving the problem of indwelling needle fixation, and it could potentially improves the success rate of puncture. Based on our experience, retrograde puncture is more suitable for elderly patients, patients with septic tumors, and patients with shock etc.
References
- Ding Wei. Progress in the prevention and care of patients with chemotherapy-induced phlebitis in cancer patients. Chinese Journal of Clinicians. 2018; 1-2. (in Chinese).
- Wei Guihua, Huang Jian, Xie Xiaohua. The application of retrograde venous puncture in the distal limbs of superficial veins in clinical practice. Chinese modern doctor. 2015; 4:152-154. (in Chinese).
- Shao Meixia, Jiang Qin. Retrograde venipuncture in elderly patients with chronic diseases. J. China Practical Medicine. 2014; 32:215-215. (in Chinese).
- Li Yuxia, Chen Yinping. Intravenous indwelling needle retrograde venipuncture in the application of infusion . Xinjiang Traditional Chinese Medicine. 2015; 33(2):55-56. (in Chinese).
- Cai Hongjing. The effect of acral joint retrograde puncture infusion and fixation method. J. China Practical Medicine. 2015; 18: 263-264. (in Chinese).
- Jiao Yuan. Application of retrograde venous puncture in the hand for clinical infusion in elderly patients. Shanxi Medical Journal. 2017; 22. (in Chinese).
- Zhou Wei-xiang. Application of retrograde venous puncture in the hand in elderly patients infusion. Journal of Preventive Medicine of the Straits. 2016; 05. (in Chinese).